Written by Mark W. Parrino, MPA – AATOD President
April 27, 2017
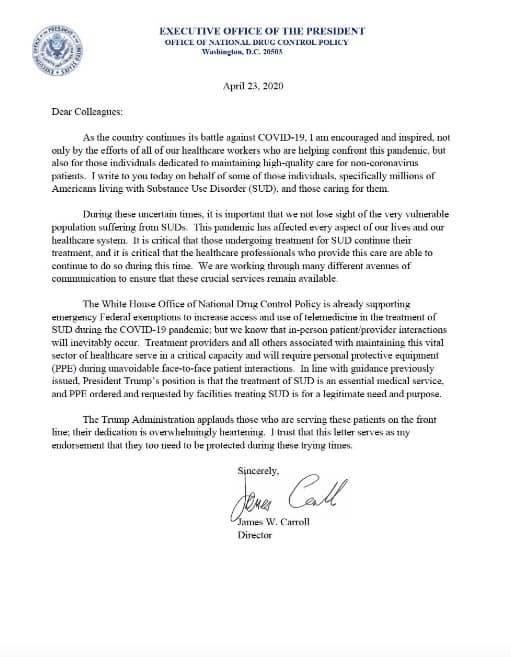
As many of our readers know, it has been impossible to pick up a paper or watch television news without hearing a story about the current opioid addiction crisis in America. President Trump recently appointed Governor Christie to be the head of the Commission, focusing on addiction and the opioid crisis. Additionally, HHS Secretary Price nominated Dr. Elinore McCance-Katz to serve as the Assistant Secretary for Mental Health and Substance Use in HHS. Both of these appointments are excellent and will be extremely beneficial to our field.
Congress approved the CURES funding package and SAMHSA is currently working with the states and grantees to utilize the first $500 million dollars of funding in 2017.
Some states have extremely innovative models, such as the Vermont Hub and Spoke model. While other states have been challenged in providing access to treatment for their state residents. We have just learned that the state of Mississippi is expanding access to OTPs in order to get the patients the care they need. In the past several years, a large number of Mississippi residents have crossed the border to access care in Alabama and Louisiana. This is welcome news and we are grateful for such a progressive turn in the state’s approach to treatment.
We also know that a number of Tennessee residents cross the border to access care in northwestern Georgia. This border crossing caused the Georgia legislature to impose a moratorium on opening new OTPs. This moratorium is expected to be lifted at the end of the current calendar year as the legislature wraps up its findings.
The Commissioner of Health for West Virginia, Dr. Rahul Gupta, recently expressed his interest in developing a comprehensive plan to reduce the number of opioid related deaths in his state. I recently wrote Dr. Gupta, urging him to lift the longstanding moratorium, which has prevented the development of new OTPs in West Virginia since 2008.
While we are in an age of conflicting interests and a growing sense of urgency in order to protect our citizens from the ravages of opioid addiction, we also need to be clear in following evidence based practices and effective policies. Regardless of the state you live in, we need a balance of well-coordinated efforts with prevention, treatment and enforcement. These have always been the three essential policy cornerstones for any effective policy in this field.
We also need to be careful about advancing one addiction treatment medication at the expense of another. There are only three federally approved medications to treat opioid addiction. They all have value and they all should be used at different times in the experience of patient care depending on what the individual needs. Illustratively, Vivitrol (Naltrexone) represents an excellent medication for a former opioid addicted inmate, who has been in jail for some time and is about to be released. Many inmates generally have a fear of relapse upon release from long term incarceration even though they have not used opioids for some time. There are a number of correctional facilities that are using Vivitrol injections before the inmate is released. Once again, the key here is to ensure that the patient gets access to a referral so that they can continue their treatment with Vivitrol or other medications, which are deemed medically appropriate and effective. A number of correctional facilities are also working with treatment providers so that inmates with opioid use disorders get access to methadone and buprenorphine.
While methadone maintenance is still considered the “gold standard” of medications to treat this disorder, there are a number of people who have forgotten that it exists and do not factor it into their plan to treat this disorder. The state of Wyoming comes to mind as the recent recipient of a SAMHSA grant. A recent newspaper story indicated that such treatment providers do not believe that methadone is a safe medication to treat this disorder.
Buprenorphine is an excellent medication and access to such medication has increased through DATA 2000 practices. Once again, all of these medications should be used with effective and well-coordinated services.
Ultimately, there will be many discussions about what works best for patients and how the system should function in an integrated way. The only way we are going to get a handle in dealing with an epidemic that has taken 25 years to develop, is to be clear in setting realistic goals about what can be done.
Finally, financial and workforce resources also need to be available as treatment access increases.






























{kind=link}